
 The reason MMS1 can get further into the intestinal tract then CDS... by Tara W
The reason MMS1 can get further into the intestinal tract then CDS... by Tara W
- CLO2
-
 Topic Author
Topic Author
- Offline
- Administrator
-

Less
More
02 Dec 2024 13:51 - 08 Dec 2024 08:17 #84917
by CLO2
The reason MMS1 can get further into the intestinal tract then CDS... by Tara W was created by CLO2
Forwarded from Tara W (Telegram) [02-Dec-24 05:13]
The reason MMS1 can get further into the intestinal tract than CDS has a lot to do with the anatomy/physiology of the gastrointestinal tract, and the chemical make up of CDS and MMS1.
I am not a biologist or a chemist, so this is my “layman’s explanation” of how the processes are different. 😊
As far as the physiology…
When a gas is “put into” or “created” in the stomach, it can penetrate the stomach wall and go directly into the bloodstream.
However, the absorption of liquids through the stomach wall is negligible. Most liquids don’t start getting absorbed until they pass through the stomach and enter the small intestine.
Regarding the properties of CDS, MMS1, and MMS…
CDS is chlorine dioxide gas infused into water. CDS is a “complete product,” and, once it’s made it will only get weaker. To make CDS, CLO2 gas was forced into a surrounding liquid, and it constantly wants to come back out of that liquid.
MMS1, on the other hand, is a combination of two liquid mixtures…for my example, a diluted hydrochloric acid (HCL) solution and the sodium chlorite solution (SCS). When SCS solution and HCL are mixed together, they’re only 10% activated in that mixture. This means only ~10% of the sodium chlorite molecules and the acid molecules will have “bumped into each other” to create CLO2 gas. Adding water to a dose for proper dilution further separates the molecules and slows down the activation process. (They cannot “activate” unless they can bump into each other.) Adequate stomach acid can provide a “boost” to help activate the sodium chlorite molecules in an MMS1 dose even faster.
When CLO2 gas molecules hit a “pathogen, diseased tissue, specific amino acid, lactic acid, sulfur-based molecule, antioxidant, enzyme, etc,” the gas is converted to salt and water.
As far as digestion goes…
When CDS is put into a warm, empty stomach, the CLO2 gas quickly comes out of the CDS and moves through the stomach wall into the bloodstream. The remaining water then moves into the intestinal tract (within ~5 minutes), where it is absorbed.
When MMS1 is put into a warm, empty stomach, remember, it’s only 10% activated. It continues to activate, but not all of it can become activated in ~5 minutes. So, when the stomach moves an MMS1 dose into the small intestine for absorption, there is still inactivated sodium chlorite in that mixture. Once in the intestinal tract, some of that inactivated sodium chlorite is absorbed into the bloodstream, while some is carried further down the intestinal tract. Inactivated SCS in the bloodstream or intestinal tract can be activated into chlorine dioxide if it bumps into some type of activating acid.
If someone has a larger or “neutralizing” meal in their stomach when they take a CDS dose, the CLO2 will likely not travel beyond the stomach. As heavy meals are being churned in a warm stomach during digestion, which can take ~2 - 4 hours, some CLO2 gas molecules can get through the stomach wall, but others will bump into “pathogens, diseased tissues, specific amino acids, sulfur-based molecules, antioxidants, enzymes, etc.,” and can be neutralized. With CDS and a meal, only a fraction of the CLO2 will make it through the stomach wall, as compared to an empty stomach.
For somebody using either MMS or MMS1 as their form of chlorine dioxide, both of which contain inactivated sodium chlorite, small or neutral snacks can still provide an opportunity for sodium chlorite to get into the small intestine and have therapeutic benefits beyond the stomach. Because both of these forms of chlorine dioxide are not fully activated when ingested, they continue to activate and produce CLO2, even with food in the stomach. In my opinion, this is why MMS or MMS1 doses are “more forgiving” with food than CDS is.
So, imo, the ability for chlorine dioxide to move beyond the stomach and into the intestinal tract depends both on the form of the chlorine dioxide, and the contents of the stomach.
The reason MMS1 can get further into the intestinal tract than CDS has a lot to do with the anatomy/physiology of the gastrointestinal tract, and the chemical make up of CDS and MMS1.
I am not a biologist or a chemist, so this is my “layman’s explanation” of how the processes are different. 😊
As far as the physiology…
When a gas is “put into” or “created” in the stomach, it can penetrate the stomach wall and go directly into the bloodstream.
However, the absorption of liquids through the stomach wall is negligible. Most liquids don’t start getting absorbed until they pass through the stomach and enter the small intestine.
Regarding the properties of CDS, MMS1, and MMS…
CDS is chlorine dioxide gas infused into water. CDS is a “complete product,” and, once it’s made it will only get weaker. To make CDS, CLO2 gas was forced into a surrounding liquid, and it constantly wants to come back out of that liquid.
MMS1, on the other hand, is a combination of two liquid mixtures…for my example, a diluted hydrochloric acid (HCL) solution and the sodium chlorite solution (SCS). When SCS solution and HCL are mixed together, they’re only 10% activated in that mixture. This means only ~10% of the sodium chlorite molecules and the acid molecules will have “bumped into each other” to create CLO2 gas. Adding water to a dose for proper dilution further separates the molecules and slows down the activation process. (They cannot “activate” unless they can bump into each other.) Adequate stomach acid can provide a “boost” to help activate the sodium chlorite molecules in an MMS1 dose even faster.
When CLO2 gas molecules hit a “pathogen, diseased tissue, specific amino acid, lactic acid, sulfur-based molecule, antioxidant, enzyme, etc,” the gas is converted to salt and water.
As far as digestion goes…
When CDS is put into a warm, empty stomach, the CLO2 gas quickly comes out of the CDS and moves through the stomach wall into the bloodstream. The remaining water then moves into the intestinal tract (within ~5 minutes), where it is absorbed.
When MMS1 is put into a warm, empty stomach, remember, it’s only 10% activated. It continues to activate, but not all of it can become activated in ~5 minutes. So, when the stomach moves an MMS1 dose into the small intestine for absorption, there is still inactivated sodium chlorite in that mixture. Once in the intestinal tract, some of that inactivated sodium chlorite is absorbed into the bloodstream, while some is carried further down the intestinal tract. Inactivated SCS in the bloodstream or intestinal tract can be activated into chlorine dioxide if it bumps into some type of activating acid.
If someone has a larger or “neutralizing” meal in their stomach when they take a CDS dose, the CLO2 will likely not travel beyond the stomach. As heavy meals are being churned in a warm stomach during digestion, which can take ~2 - 4 hours, some CLO2 gas molecules can get through the stomach wall, but others will bump into “pathogens, diseased tissues, specific amino acids, sulfur-based molecules, antioxidants, enzymes, etc.,” and can be neutralized. With CDS and a meal, only a fraction of the CLO2 will make it through the stomach wall, as compared to an empty stomach.
For somebody using either MMS or MMS1 as their form of chlorine dioxide, both of which contain inactivated sodium chlorite, small or neutral snacks can still provide an opportunity for sodium chlorite to get into the small intestine and have therapeutic benefits beyond the stomach. Because both of these forms of chlorine dioxide are not fully activated when ingested, they continue to activate and produce CLO2, even with food in the stomach. In my opinion, this is why MMS or MMS1 doses are “more forgiving” with food than CDS is.
So, imo, the ability for chlorine dioxide to move beyond the stomach and into the intestinal tract depends both on the form of the chlorine dioxide, and the contents of the stomach.
Last edit: 08 Dec 2024 08:17 by CLO2.
The following user(s) said Thank You: JimH1954, Jnana, healthfreedom79, Yodalove
Please Log in or Create an account to join the conversation.
- gertler
-

- Offline
- New Member
-

Less
More
- Posts: 13
- Thank you received: 7
13 Dec 2024 01:47 #84983
by gertler
Replied by gertler on topic The reason MMS1 can get further into the intestinal tract then CDS... by Tara W
What is the difference between MMS and MMS1?
Please Log in or Create an account to join the conversation.
- CLO2
-
Topic Author
- Offline
- Administrator
-
13 Dec 2024 10:47 #84986
by CLO2
Replied by CLO2 on topic The reason MMS1 can get further into the intestinal tract then CDS... by Tara W
Please see attached PDF files and share them with others.
The definitions for MMS came from Jim Humble. You should read his 2019 book.
The definitions for MMS came from Jim Humble. You should read his 2019 book.
The following user(s) said Thank You: JimH1954
Please Log in or Create an account to join the conversation.
- JimY
-
- Offline
- Junior Member
-

Less
More
- Posts: 37
- Thank you received: 9
19 Dec 2024 20:25 #85078
by JimY
Replied by JimY on topic The reason MMS1 can get further into the intestinal tract then CDS... by Tara W
Does this mean MMS1 is better than CDS if people can't keep their stomach empty during the day.
If I use 120ml boston bottle with PP/PE caps, can I put activated MMS (MMS1) into 8 x 120ml bottles and it won't lose potency during the day?
What about the glass bottle with stainless steel cap with silicone seal? Are they compatible with activated MMS? (I would imagine not as there are still acid and alkaline in it)
If I use 120ml boston bottle with PP/PE caps, can I put activated MMS (MMS1) into 8 x 120ml bottles and it won't lose potency during the day?
What about the glass bottle with stainless steel cap with silicone seal? Are they compatible with activated MMS? (I would imagine not as there are still acid and alkaline in it)
Please Log in or Create an account to join the conversation.
- CLO2
-
Topic Author
- Offline
- Administrator
-
20 Dec 2024 02:39 - 20 Dec 2024 02:52 #85081
by CLO2
Replied by CLO2 on topic The reason MMS1 can get further into the intestinal tract then CDS... by Tara W
Does this mean MMS1 is better than CDS if people can't keep their stomach empty during the day. That is one reason why MMS1 could be the better choice for ingesting CLO2.
If I use 120ml Boston bottle with PP/PE caps, can I put activated MMS (MMS1) into 8 x 120ml bottles and it won't lose potency during the day? I often suggest doing that.
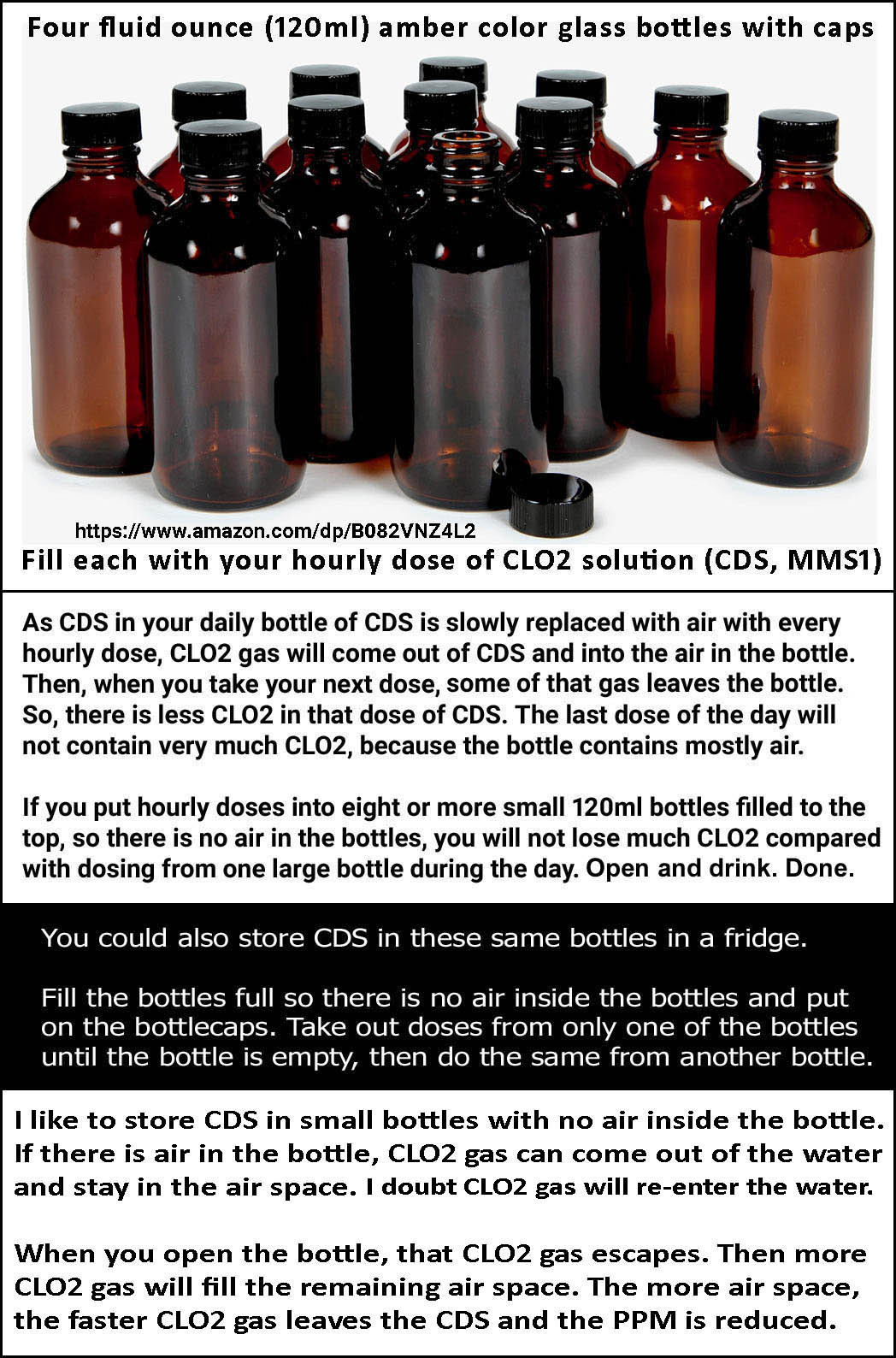
What about the glass bottle with stainless steel cap with silicone seal? Are they compatible with activated MMS? (I would imagine not as there are still acid and alkaline in it) If the silicone seal is a disc, that should be fine. Although some caps have stainless steel only on the outside of the cap, some do have SS on the inside of the cap, too. 316 stainless steel should be fine with CDS, but not with MMS1.
Last edit: 20 Dec 2024 02:52 by CLO2.
The following user(s) said Thank You: JimH1954, JimY
Please Log in or Create an account to join the conversation.
- Yodalove
-
- Offline
- New Member
-
Less
More
- Posts: 8
- Thank you received: 2
23 Mar 2025 22:00 #86010
by Yodalove
Replied by Yodalove on topic The reason MMS1 can get further into the intestinal tract then CDS... by Tara W
Brava! So does your post also explain why a well-preserved sample of CDS is more effective when used topically than MMS1—because MMS1 outside the body is only 10% sodium chlorite?
Please Log in or Create an account to join the conversation.
Time to create page: 0.238 seconds
The MMS HEALTH RECOVERY GUIDEBOOK is Jim’s latest book. It provides the latest information on how to safely use MMS. Click the book image to order your copy today.
Jim's Blog
Feed not found.